Solving referral challenges for urban poor to access Emergency Obstetric and New-born Care
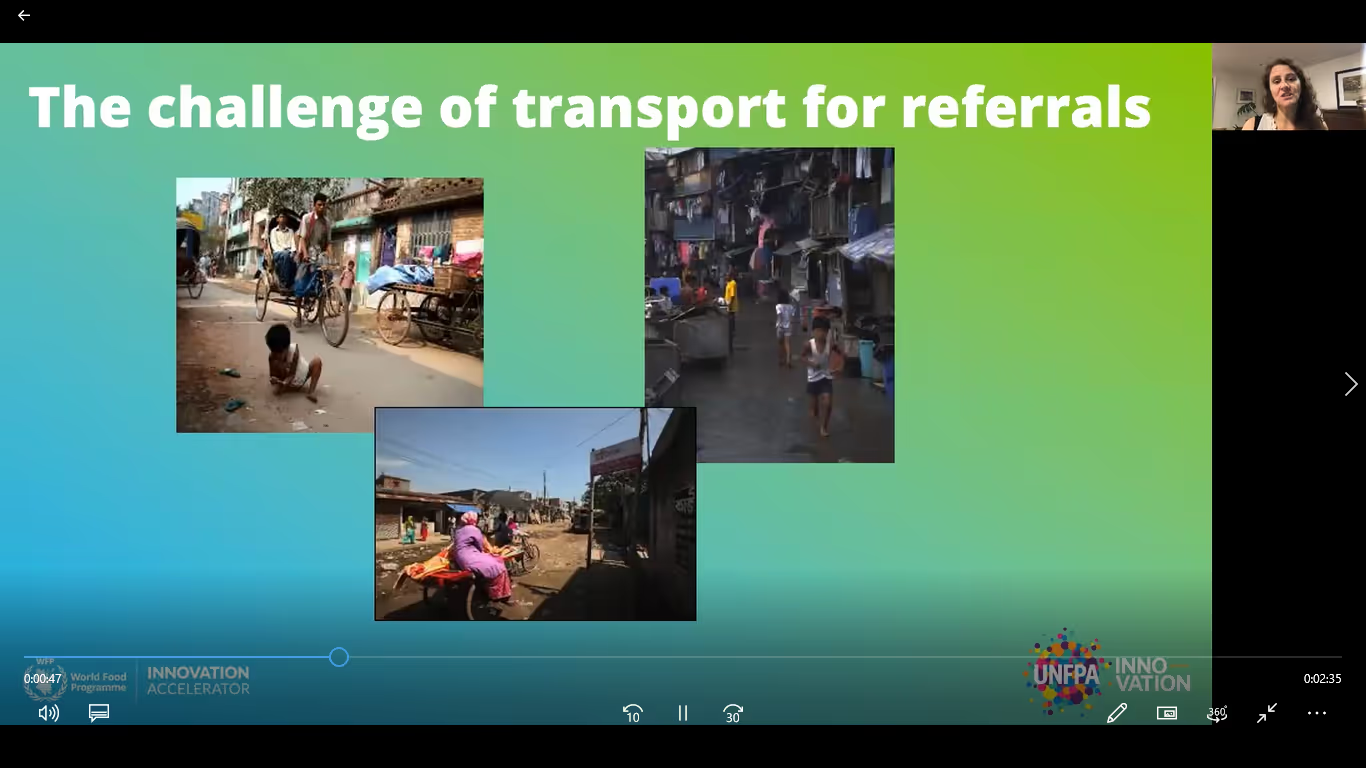
The problem: Women and adolescent childbearing girls living in the slums in Bangladesh lack financial and geographic access to an evidence-based, timely, referral process from the midwifery centre to a specific referral hospital when required for continued management of high risk pregnant women and obstetric emergencies. Currently, there is no systematic process in place (from the midwifery centre to a specific hospital) with a dependable transport method and communication pathway. This results in childbearing women and adolescents experiencing a lack of access to comprehensive emergency obstetric and new-born care (CEmONC), maternal and new-born morbidity and mortality, and increasing impoverishment. Approximately 15-20% of women experience some type of complication during labour that requires a higher level of care. This is compounded in the slums where there is low use of facility-based birth, higher rates of maternal mortality compared to national average, and a lack of standardization for operations and communication. Size and importance of the problem: In Bangladesh, the urban population is rapidly increasing from 23% in 2011, to 37.2% in 2019, and is projected to be 55.7% by 2050. Only 13% of the slum dwellers have easy and affordable access to health care facilities. Additionally, because of Bangladesh’s lack of UHC and high out of pocket costs, slum dwellers have limited access to healthcare. Less than half of all deliveries take place in health care facilities due to preference for home environment, poor quality of care and disrespect and abuse at health care facilities, as well as fear of potential surgery and costs. To summarize, the growing urban population in Bangladesh live in densely populated slums with limited access to facility-based birth, respectful maternity care, and comprehensive emergency obstetric and new-born care services (CEmONC) which resulted in low rates of facility-based birth as well as high rates of maternal mortality. It is not just the lack of community based health care facilities and skilled service providers providing safe and compassionate care, but additionally they lack a referral and transportation system to access higher level health facilities that can provide continued quality emergency care when needed that is dignified, financially affordable and geographically accessible. This ultimately results in unsafe births without a skilled attendant, and increased maternal and new-born morbidity and mortality. Proposed solution: Our 24/7 referral platform will provide access to continued comprehensive emergency obstetric and new-born care services when needed at the referral hospital for women by reducing the delay in reaching the hospital and improving quality of care. Using a structured process for communication between midwife to driver, and the referring midwife and the receiving health care provider- seamless referrals and continuity of care will be provided. The main users of our platform are the midwives working in the midwifery centres and the transport drivers, both in the urban slum areas of Dhaka in Bangladesh, as well as the receiving health care provider at the referral facility. However, the pregnant women are the main beneficiaries of this intervention. How this solution is different: Currently there is no structured, designated referral pathway or service available. Therefore, the proposed solution is the pioneer and unique one and as such, cannot be compared with others. By engaging the three parts of a successful referral- the midwife, driver and receiving health care provider we create a comprehensive system that engages the users and strengthens the quality of care with the improved communication and efficiency. Vision for the project: We envision that all women living in the urban slums in Bangladesh have access to 24/7 dignified, quality and evidence-based delivery services- including comprehensive emergency services when needed- without any financial and geographical barriers to access. This will only happen when there is a strong referral system in place to seamlessly refer from midwifery centre to the nearest CEmOC facilities both Public and Private with free and/or subsidized services, that is with affordable cost. To this goal, we would like to scale up Midwifery led Delivery Centre in Slums with clinical practice guidelines and operational standards, linked to a structured referral system. This we believe will significantly improve maternal health status of the urban slum women in Bangladesh. Contribution to UHC: The proposed innovation ensures equitable access to quality maternal health care for the women in slum populations, realizing their rights. It reduces preventable mortality and morbidity and minimizes the health, financial and economic burden on families and communities. Under the innovative financing model, where the private sector will provide free and subsidized services in exchange for evidenced based referrals, will reduce out-of-pocket spending and the catastrophic impact of health care on the poor. Lastly, it will contribute to the realisation of 3 zeros with special focus to zero preventable maternal mortality while zero unmet need for family planning, and zero gender-based violence are the ultimate outcomes.

.avif)